Really? doing nothing is an option? Charge them $1000 a dead neuron, that will concentrate the mind. You're supposed to do no harm, dead neurons are considered harm, aren't they?
Acute Ischemic Stroke With Mild Symptoms–To Thrombolyse or Not to Thrombolyse?
 Julia Ferrari
Julia Ferrari Audrey Reynolds
Audrey Reynolds Michael Knoflach3 and
Michael Knoflach3 and - 1Department of Neurology, St John's Hospital, Vienna, Austria
- 2Department of Neurology, St Vincent's University Hospital, Dublin, Ireland
- 3Department of Neurology, Medical University of Innsbruck, Innsbruck, Austria
- 4Medical Faculty, Sigmund Freud University Vienna, Vienna, Austria
Management of stroke with minor symptoms may represent a therapeutical dilemma as the hemorrhage risk of acute thrombolytic therapy may eventually outweigh the stroke severity. However, around 30% of patients presenting with minor stroke symptoms are ultimately left with disability. The objective of this review is to evaluate the current literature and evidence regarding the management of minor stroke, with a particular emphasis on the role of IV thrombolysis. Definition of minor stroke, pre-hospital recognition of minor stroke and stroke of unknown onset are discussed together with neuroimaging aspects and existing evidence for IV thrombolysis in minor strokes. Though current guidelines advise against the use of thrombolysis in those without clearly disabling symptoms due to a paucity of evidence, advanced imaging techniques may be able to identify those likely to benefit. Further research on this topic is ongoing.
Introduction
A scenario known to every neurologist: a patient with acute onset mild stroke symptoms is admitted to the hospital. Imaging excludes an intracranial hemorrhage. Should intravenous thrombolysis be given? What are the risks and what are the benefits? It is frequently assumed that for those with mild stroke symptoms, risks of thrombolysis outweigh potential benefits. However, despite having “minor” symptoms, one-third of stroke patients were not functionally independent at 90 days when considered too mild to treat for intravenous thrombolysis (1–4). The purpose of this review is to provide an update on the acute treatment of patients with minor stroke with a special focus on intravenous thrombolysis.
Definition of Stroke With Mild Symptoms
The definition of a stroke with mild symptoms or minor stroke (MS) is not standardized. Definitions are often based on the National Institutes of Health Stroke Scale (NIHSS) requiring a score ≤ 1 on every item (5) or utilize certain limits, mostly NIHSS ≤ 6 (6). Other definitions include whether symptoms are disabling or non-disabling, e.g., isolated aphasia or a severe distal paresis of the arm will give a low NIHSS score but are very disabling symptoms.
Further questions arise in differentiating minor stroke from a transient ischemic attack (TIA). In the acute phase, it is not possible to tell whether symptoms will persist or resolve spontaneously. The definition of a TIA from the American Heart and the American Stroke Association from 2002, “a transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction” (7) implies the use of an advanced imaging method to differentiate between TIA and minor stroke. This definition will build the basis for the 11th International Classification of Diseases (8). A majority of TIAs are of short duration, and once neurological deficits persist longer than 60 min they resolve in <15% within 24 h (9). Furthermore, only 2% of patients that received placebo in the National Institute of Neurological Disorders and Stroke rt-PA Stroke Study were free of symptoms 24 h later (10).
Those with rapidly improving symptoms are usually excluded from receiving thrombolysis therapy. Rapidly improving symptoms are those which improve spontaneously after presentation, but the definition is ambiguous. However, their outcomes are not predictable, with 30% of those with minor stroke or rapidly improving symptoms not fully functionally independent at hospital discharge (1).
Disabling or Non-Disabling Symptoms?
Determining whether symptoms are “disabling” or not is an important factor in the management of acute MS. A pooled metanalysis of nine trials could show that thrombolysis treatment resulted in a nearly 10% better chance of an excellent functional outcome after 3 months in patients with clearly disabling deficits such as aphasia or hemiparesis (11, 12).
For those with non-disabling symptoms, however, less evidence exists. Only one of these nine trials–the Third International Stroke Trial (IST-3) (13)–did not exclude patients with non-disabling symptoms.
IST-3 found evidence of benefit for thrombolysis for those presenting within 6 h of symptoms of stroke, however the benefit increased with increasing NIHSS and was less beneficial for those with minor stroke symptoms. Out of the 106 patients randomized with NIHSS ≤ 5, 60% showed a favorable outcome after 3 months.
Non-disabling symptoms include transient, fluctuating or persistent symptoms without unilateral motor weakness or language/speech disturbance (e.g., hemi-body sensory symptoms, monocular vision loss, binocular diplopia, hemifield vision loss, dysarthria, dysphagia, or ataxia). The PRISMS trial, a randomized controlled trial (RCT), showed that among patients with a low NIHSS and no disabling deficit, rtPA may not provide a benefit and might increase the risk of symptomatic intracranial hemorrhage (6). A clearly disabling deficit was operationally defined as a deficit that, if unchanged, would prevent the patient from performing basic activities of daily living (i.e., bathing, ambulating, toileting, hygiene, and eating) or returning to work. Judging how disabling a deficit will be in the future is challenging in the hyperacute stroke setting.
A further obstacle to thrombolysis treatment in minor stroke is that patients with minor stroke symptoms do not receive the priority of emergency medical services and in-hospital triage pathways leading to relevant time delays in onset-to-door and door-to-imaging times (14).
Prehospital Recognition of Minor Stroke
The presentation of those with mild symptoms is frequently delayed compared to major stroke as it may not be recognized in the acute phase, leading to undertreatment. Public knowledge of stroke symptoms according to the FAST campaign is only about 70%, with the highest rate found in females and in the older and white population (15). Additionally, the mode of arrival at the hospital plays an important role. Patterns of emergency medical services pre-notification vary across countries. Data from a cohort study in New York showed that patients with minor stroke have longer door to needle times if the mode of arrival was without pre-notification (16).
The clinical significance of posterior circulation symptoms is often not recognized and, therefore, mostly remain undertreated in the acute phase. As in the NIHSS symptoms of the posterior circulation are underrepresented (e.g., vertigo, imbalance of gait), strokes in this territory are more likely to be defined as “minor” if a cut-off NIHSS score is used.
Wake up Stroke and Stroke of Unknown Onset
Those who wake up with stroke were traditionally excluded from revascularization therapies, due to unknown time of onset. Due to circadian rhythms there is diurnal variation in stroke onset, with a higher number occurring in the morning, which may be related to a surge in blood pressure (17). This suggests that the stroke may have occurred shortly before awakening, though the true time of onset is unknown. Modern imaging technologies, such as MRI DWI and FLAIR mismatch and or perfusion imaging, can help identify those who may benefit from thrombolysis or thrombectomy (18). The WAKE-UP trial showed that those with strokes evident from sleep with favorable MRI findings (DWI and FLAIR mismatch) who were treated with IV alteplase had significantly better functional outcomes, though more intracranial hemorrhages, than placebo at 90 days (19). The WAKE-UP trial included patients with all types of stroke severity, but the median NIHSS was of mild to moderate severity (median NIHSS 6, interquartile range 4–9). Analysis of patients with minor stroke has not been reported so far. Penumbral pattern identified using perfusion imaging is another recent radiological paradigm to identify those to benefit from reperfusion in the absence of onset time knowledge. Trials including ECASS4, EPITHET and EXTEND proved positively this concept for wake-up strokes and extended time window (4.5–9 h) thrombolysis (20).
Thrombolysis for wake-up stroke with minor symptoms has not been specifically studied. As mentioned previously, many stroke centers do not perform advanced imaging in those with NIHSS ≤ 6, and may be missing those with mismatch deficits or large vessel occlusions who could potentially benefit from thrombolysis. See also illustrative patient case in Figure 2.
Current Evidence of use of Thrombolytic Agents in Patients With Minor Stroke
Current guidelines and recommendations state that for patients with acute minor disabling ischemic stroke of <4.5 h duration, intravenous thrombolysis with recombinant alteplase is recommended/ may be reasonable (21, 22). RCTs and observational studies addressing this topic so far showed promising results with a good functional outcome and a low complication rate (Table 1).
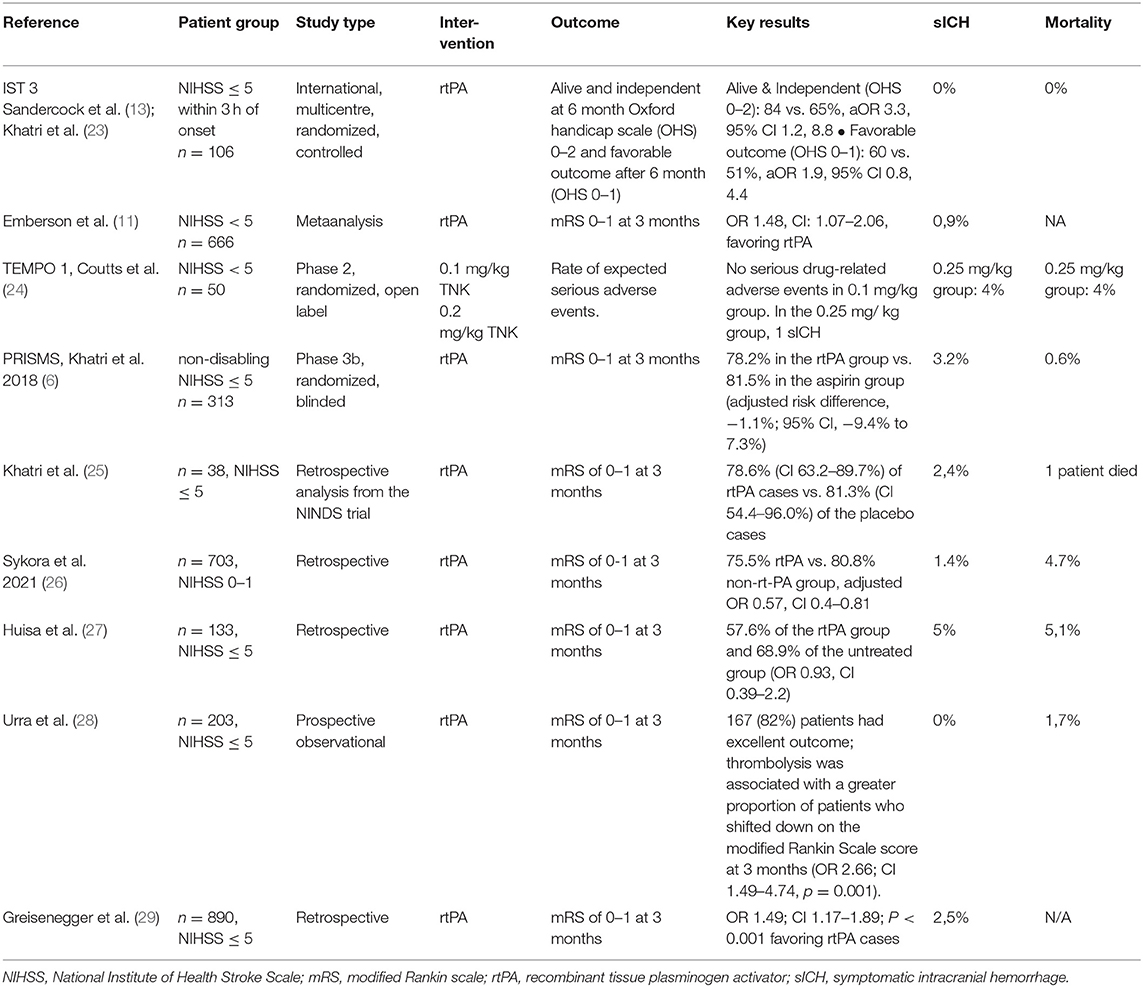
Table 1. Randomized controlled trials and observational trials on thrombolysis in minor stroke.
For patients with acute minor non-disabling ischemic stroke of <4.5 h duration, no intravenous thrombolysis is recommended. One exception may be patients with non-disabling symptoms and a large vessel occlusion. However, many acute stroke centers do not perform angiography for those with NIHSS <6 as part of their internal protocol, and many centers do not have access to advanced imaging such as CT perfusion. Therefore, an unknown proportion of stroke with minor symptoms who have large vessel occlusions amenable to intervention are being missed. TEMPO 1, a case series of 50 patients with mild symptoms and intracranial vessel occlusion, which showed that administration of tenecteplase-tissue-type plasminogen activator in minor stroke with intracranial occlusion is feasible and safe (24). Wang et al. found that intravenous thrombolysis benefits though with mild stroke symptoms (NIHSS ≤ 5) and large artery atherosclerosis, though not those who had a tandem proximal intracranial occlusion and cervical internal artery lesion (complete occlusion or severe stenosis ≥ 90%) (30). They found that LAA-type patients (as defined by TOAST criteria) had significantly favorable outcomes after treatment with thrombolysis compared to untreated patients, however no such benefits were observed in other stroke subtypes, such as cardioembolic, small vessel occlusion and undetermined. This suggests that CT or MR angiography might be helpful to choose patients for thrombolysis that present with stroke with minor symptoms.
Alteplase or Tenecteplase in Patients With Minor Stroke
In recent years, the recombinant plasminogen activator tenecteplase is increasingly competing with the gold standard alteplase. The first publication of the EXTEND IA TNK study showed that higher perfusion rates and better clinical results can be achieved with tenecteplase in the 0.25 mg/kg dose than with alteplase in patients with an acute ischemic stroke (31). Tenecteplase was used as so-called bridging thrombolysis in the 4.5 h time window until the mechanical thrombectomy was performed. In addition, tenecteplase has advantages in handling, as it can be administered as single intravenous bolus and does not require a continuous infusion over 1 h, as alteplase does. The results of the EXTEND TNK study prompted the authors of the US guideline and the European Stroke Organization (ESO) to include tenecteplase in their recommendation as an alternative fibrinolytic (AHA/ASA Class IIb recommendation), although the AHA/ASA recommendation can also be considered to the 0.4 mg/kg dose for patients with less severe neurological impairments and if there are no large vessel occlusions (Level of Evidence: IIb) (22).
The second part of the EXTEND TNK study was recently published (32) which evaluated different doses of tenecteplase. The higher dose of tenecteplase (0.4 mg/kg) did not have any disadvantages in terms of safety: there were 16 and 22 death in the high and low dose groups, respectively. Symptomatic intracerebral hemorrhages 36 h after thrombolysis were numerically more frequent in the high dose group (7 vs. 2 patients), but four bleeding events in this group were associated with wire perforations during the endovascular procedure and were therefore not attributable to thrombolysis directly. The authors of the study report that the latter results are in contrast to an earlier study with the 0.40 mg/kg dose that was terminated prematurely for safety reasons, as some patients developed symptomatic intracranial hemorrhage. As a limitation, Campbell and colleagues point out that the study may not have been powered to reveal differences in efficacy. There was no restriction on clinical severity using NIHSS scores in these trials, but showed that probably a higher perfusion rate can be achieved with tenecteplase in patients with vessel occlusions. TEMPO 2 is an ongoing multicentre prospective randomized open label blinded-endpoint (PROBE) controlled trial of thrombolysis with low dose TEnecteplase vs. standard of care in Minor ischemic stroke with Proven acute symptomatic Occlusion (33). The hypothesis is that patients with mild (NIHSS < = 5) or even non-disabling symptoms due to identifiable vessel occlusion will benefit from IVT as compared to standard antiplatelet therapy. Results are expected in 2024. In summary, currently no evidence exists that tenecteplase should be preferred to alteplase in acute treatment of minor stroke patients, though further research is ongoing.
No comments:
Post a Comment